
Page 989 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 989
Occupational‐Related Lameness Conditions 955
VetBooks.ir
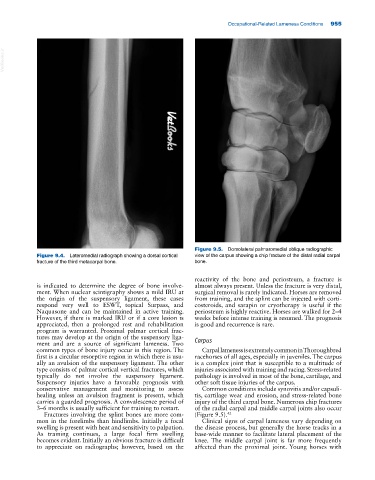
Figure 9.5. Dorsolateral palmaromedial oblique radiographic
Figure 9.4. Lateromedial radiograph showing a dorsal cortical view of the carpus showing a chip fracture of the distal radial carpal
fracture of the third metacarpal bone. bone.
reactivity of the bone and periosteum, a fracture is
is indicated to determine the degree of bone involve almost always present. Unless the fracture is very distal,
ment. When nuclear scintigraphy shows a mild IRU at surgical removal is rarely indicated. Horses are removed
the origin of the suspensory ligament, these cases from training, and the splint can be injected with corti
respond very well to ESWT, topical Surpass, and costeroids, and sarapin or cryotherapy is useful if the
Naquasone and can be maintained in active training. periosteum is highly reactive. Horses are walked for 2–4
However, if there is marked IRU or if a core lesion is weeks before intense training is resumed. The prognosis
appreciated, then a prolonged rest and rehabilitation is good and recurrence is rare.
program is warranted. Proximal palmar cortical frac
tures may develop at the origin of the suspensory liga Carpus
ment and are a source of significant lameness. Two
common types of bone injury occur in this region. The Carpal lameness is extremely common in Thoroughbred
first is a circular resorptive region in which there is usu racehorses of all ages, especially in juveniles. The carpus
ally an avulsion of the suspensory ligament. The other is a complex joint that is susceptible to a multitude of
type consists of palmar cortical vertical fractures, which injuries associated with training and racing. Stress‐related
typically do not involve the suspensory ligament. pathology is involved in most of the bone, cartilage, and
Suspensory injuries have a favorable prognosis with other soft tissue injuries of the carpus.
conservative management and monitoring to assess Common conditions include synovitis and/or capsuli
healing unless an avulsion fragment is present, which tis, cartilage wear and erosion, and stress‐related bone
carries a guarded prognosis. A convalescence period of injury of the third carpal bone. Numerous chip fractures
3–6 months is usually sufficient for training to restart. of the radial carpal and middle carpal joints also occur
Fractures involving the splint bones are more com (Figure 9.5). 42
mon in the forelimbs than hindlimbs. Initially a focal Clinical signs of carpal lameness vary depending on
swelling is present with heat and sensitivity to palpation. the disease process, but generally the horse tracks in a
As training continues, a large focal firm swelling base‐wide manner to facilitate lateral placement of the
becomes evident. Initially an obvious fracture is difficult knee. The middle carpal joint is far more frequently
to appreciate on radiographs; however, based on the affected than the proximal joint. Young horses with