
Page 243 - Essential Haematology
P. 243
Chapter 17 Acute lymphoblastic leukaemia / 229
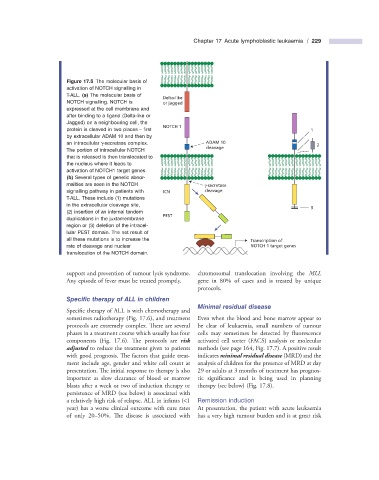
Figure 17.5 The molecular basis of
activation of NOTCH signalling in
T - ALL. (a) The molecular basis of
Delta-like
NOTCH signalling. NOTCH is or jagged
expressed at the cell membrane and
after binding to a ligand (Delta - like or
Jagged) on a neighbouring cell, the
NOTCH 1
protein is cleaved in two places – fi rst 1
by extracellular ADAM 10 and then by
an intracellular γ - secretase complex. ADAM 10 2
cleavage
The portion of intracellular NOTCH
that is released is then translocated to
the nucleus where it leads to
activation of NOTCH1 target genes.
(b) Several types of genetic abnor-
malities are seen in the NOTCH γ-secretase
signalling pathway in patients with ICN cleavage
T - ALL. These include (1) mutations
in the extracellular cleavage site,
3
(2) insertion of an internal tandem
PEST
duplications in the juxtamembrane
region or (3) deletion of the intracel-
lular PEST domain. The net result of
all these mutations is to increase the Transcription of
rate of cleavage and nuclear NOTCH 1 target genes
translocation of the NOTCH domain.
support and prevention of tumour lysis syndrome. chromosomal translocation involving the MLL
Any episode of fever must be treated promptly. gene in 80% of cases and is treated by unique
protocols.
Specifi c t herapy of ALL in c hildren
Minimal r esidual d isease
Specific therapy of ALL is with chemotherapy and
sometimes radiotherapy (Fig. 17.6 ), and treatment Even when the blood and bone marrow appear to
protocols are extremely complex. There are several be clear of leukaemia, small numbers of tumour
phases in a treatment course which usually has four cells may sometimes be detected by fl uorescence
components (Fig. 17.6 ). The protocols are risk activated cell sorter (FACS ) analysis or molecular
adjusted to reduce the treatment given to patients methods (see page 164, Fig. 17.7 ). A positive result
with good prognosis. The factors that guide treat- indicates minimal residual disease (MRD) and the
ment include age, gender and white cell count at analysis of children for the presence of MRD at day
presentation. The initial response to therapy is also 29 or adults at 3 months of treatment has prognos-
important as slow clearance of blood or marrow tic significance and is being used in planning
blasts after a week or two of induction therapy or therapy (see below) (Fig. 17.8 ).
persistence of MRD (see below) is associated with
a relatively high risk of relapse. ALL in infants ( < 1 Remission i nduction
year) has a worse clinical outcome with cure rates At presentation, the patient with acute leukaemia
of only 20 – 50%. The disease is associated with has a very high tumour burden and is at great risk