
Page 270 - Essential Haematology
P. 270
256 / Chapter 20 Non-Hodgkin lymphoma
Mantle cell Follicular
lymphoma lymphoma
Plasma Myeloma
cell
Germinal follicle
Mantle zone
Marginal zone
Ig isotype switch
with Ig mutations
Bone
marrow Marginal zone
lymphoma
Naive
B cells
Chronic lymphocytic Lymphoplasmacytoid
leukaemia lymphoma
Diffuse large
cell lymphoma
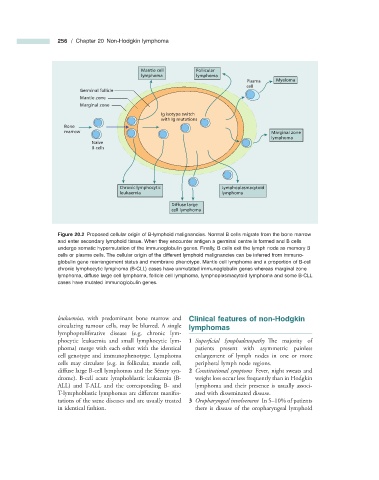
Figure 20.2 Proposed cellular origin of B - lymphoid malignancies. Normal B cells migrate from the bone marrow
and enter secondary lymphoid tissue. When they encounter antigen a germinal centre is formed and B cells
undergo somatic hypermutation of the immunoglobulin genes. Finally, B cells exit the lymph node as memory B
cells or plasma cells. The cellular origin of the different lymphoid malignancies can be inferred from immuno-
globulin gene rearrangement status and membrane phenotype. Mantle cell lymphoma and a proportion of B - cell
chronic lymphocytic lymphoma (B - CLL) cases have unmutated immunoglobulin genes whereas marginal zone
lymphoma, diffuse large cell lymphoma, follicle cell lymphoma, lymphoplasmacytoid lymphoma and some B - CLL
cases have mutated immunoglobulin genes.
leukaemias , with predominant bone marrow and Clinical f eatures of n on - Hodgkin
circulating tumour cells, may be blurred. A single l ymphomas
lymphoproliferative disease (e.g. chronic lym-
phocytic leukaemia and small lymphocytic lym- 1 Superfi cial lymphadenopathy The majority of
phoma) merge with each other with the identical patients present with asymmetric painless
cell genotype and immunophenotype. Lymphoma enlargement of lymph nodes in one or more
cells may circulate (e.g. in follicular, mantle cell, peripheral lymph node regions.
diffuse large B - cell lymphomas and the S é zary syn- 2 Constitutional symptoms Fever, night sweats and
drome). B - cell acute lymphoblastic leukaemia (B - weight loss occur less frequently than in Hodgkin
ALL) and T - ALL and the corresponding B - and lymphoma and their presence is usually associ-
T - lymphoblastic lymphomas are diff erent manifes- ated with disseminated disease.
tations of the same diseases and are usually treated 3 Oropharyngeal involvement In 5 – 10% of patients
in identical fashion. there is disease of the oropharyngeal lymphoid