
Page 69 - Essential Haematology
P. 69
Chapter 4 Iron overload / 55
(a) (b)
(c) (d)
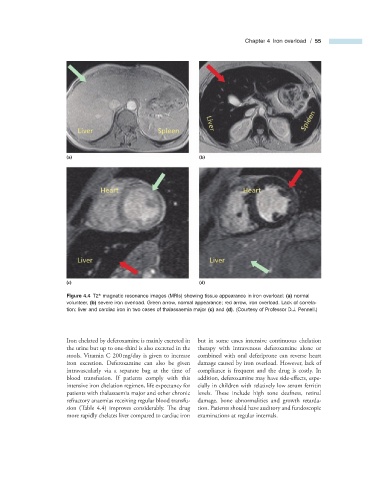
Figure 4.4 T2 * magnetic resonance images (MRIs) showing tissue appearance in iron overload: (a) normal
volunteer, (b) severe iron overload. Green arrow, normal appearance; red arrow, iron overload. Lack of correla-
tion: liver and cardiac iron in two cases of thalassaemia major (c) and (d) . (Courtesy of Professor D.J. Pennell.)
Iron chelated by deferoxamine is mainly excreted in but in some cases intensive continuous chelation
the urine but up to one - third is also excreted in the therapy with intravenous deferoxamine alone or
stools. Vitamin C 200 mg/day is given to increase combined with oral deferiprone can reverse heart
iron excretion. Deferoxamine can also be given damage caused by iron overload. However, lack of
intravascularly via a separate bag at the time of compliance is frequent and the drug is costly. In
blood transfusion. If patients comply with this addition, deferoxamine may have side - eff ects, espe-
intensive iron chelation regimen, life expectancy for cially in children with relatively low serum ferritin
patients with thalassaemia major and other chronic levels. Th ese include high tone deafness, retinal
refractory anaemias receiving regular blood transfu- damage, bone abnormalities and growth retarda-
sion (Table 4.4 ) improves considerably. Th e drug tion. Patients should have auditory and fundoscopic
more rapidly chelates liver compared to cardiac iron examinations at regular intervals.