
Page 449 - Atlas of Histology with Functional Correlations
P. 449
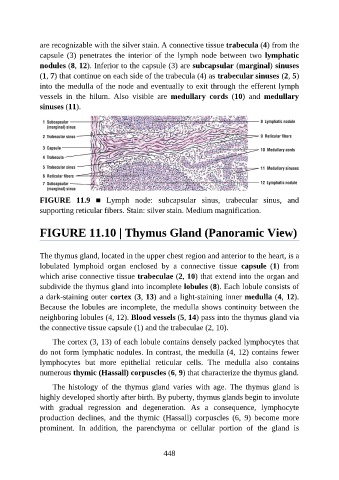
are recognizable with the silver stain. A connective tissue trabecula (4) from the
capsule (3) penetrates the interior of the lymph node between two lymphatic
nodules (8, 12). Inferior to the capsule (3) are subcapsular (marginal) sinuses
(1, 7) that continue on each side of the trabecula (4) as trabecular sinuses (2, 5)
into the medulla of the node and eventually to exit through the efferent lymph
vessels in the hilum. Also visible are medullary cords (10) and medullary
sinuses (11).
FIGURE 11.9 ■ Lymph node: subcapsular sinus, trabecular sinus, and
supporting reticular fibers. Stain: silver stain. Medium magnification.
FIGURE 11.10 | Thymus Gland (Panoramic View)
The thymus gland, located in the upper chest region and anterior to the heart, is a
lobulated lymphoid organ enclosed by a connective tissue capsule (1) from
which arise connective tissue trabeculae (2, 10) that extend into the organ and
subdivide the thymus gland into incomplete lobules (8). Each lobule consists of
a dark-staining outer cortex (3, 13) and a light-staining inner medulla (4, 12).
Because the lobules are incomplete, the medulla shows continuity between the
neighboring lobules (4, 12). Blood vessels (5, 14) pass into the thymus gland via
the connective tissue capsule (1) and the trabeculae (2, 10).
The cortex (3, 13) of each lobule contains densely packed lymphocytes that
do not form lymphatic nodules. In contrast, the medulla (4, 12) contains fewer
lymphocytes but more epithelial reticular cells. The medulla also contains
numerous thymic (Hassall) corpuscles (6, 9) that characterize the thymus gland.
The histology of the thymus gland varies with age. The thymus gland is
highly developed shortly after birth. By puberty, thymus glands begin to involute
with gradual regression and degeneration. As a consequence, lymphocyte
production declines, and the thymic (Hassall) corpuscles (6, 9) become more
prominent. In addition, the parenchyma or cellular portion of the gland is
448