
Page 12 - 2022 Benegit Guide
P. 12
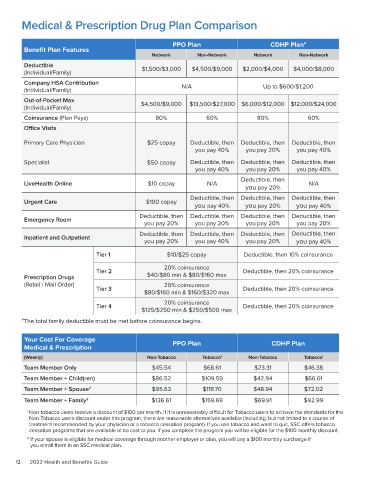
Medical & Prescription Drug Plan Comparison
PPO Plan CDHP Plan*
Benefit Plan Features
Network Non-Network Network Non-Network
Deductible $1,500/$3,000 $4,500/$9,000 $2,000/$4,000 $4,000/$8,000
(Individual/Family)
Company HSA Contribution N/A Up to $600/$1,200
(Individual/Family)
Out-of-Pocket Max $4,500/$9,000 $13,500/$27,000 $6,000/$12,000 $12,000/$24,000
(Individual/Family)
Coinsurance (Plan Pays) 80% 60% 80% 60%
Office Visits
Primary Care Physician $25 copay Deductible, then Deductible, then Deductible, then
you pay 40% you pay 20% you pay 40%
Specialist $50 copay Deductible, then Deductible, then Deductible, then
you pay 40% you pay 20% you pay 40%
Deductible, then
LiveHealth Online $10 copay N/A N/A
you pay 20%
Deductible, then Deductible, then Deductible, then
Urgent Care $100 copay
you pay 40% you pay 20% you pay 40%
Deductible, then Deductible, then Deductible, then Deductible, then
Emergency Room
you pay 20% you pay 20% you pay 20% you pay 20%
Deductible, then Deductible, then Deductible, then Deductible, then
Inpatient and Outpatient
you pay 20% you pay 40% you pay 20% you pay 40%
Tier 1 $10/$25 copay Deductible, then 10% coinsurance
20% coinsurance
Tier 2 Deductible, then 20% coinsurance
Prescription Drugs $40/$80 min & $80/$160 max
(Retail / Mail Order) 20% coinsurance
Tier 3 Deductible, then 20% coinsurance
$80/$160 min & $160/$320 max
20% coinsurance
Tier 4 Deductible, then 20% coinsurance
$125/$250 min & $250/$500 max
*The total family deductible must be met before coinsurance begins.
Your Cost For Coverage PPO Plan CDHP Plan
Medical & Prescription
(Weekly) Non-Tobacco Tobacco 1 Non-Tobacco Tobacco 1
Team Member Only $45.54 $68.61 $23.31 $46.38
Team Member + Child(ren) $86.52 $109.59 $42.94 $66.01
Team Member + Spouse 2 $95.63 $118.70 $48.94 $72.02
Team Member + Family 2 $136.61 $159.69 $69.91 $92.99
1 Non-tobacco users receive a discount of $100 per month. If it is unreasonably difficult for Tobacco users to achieve the standards for the
Non-Tobacco users discount under this program, there are reasonable alternatives available (including, but not limited to a course of
treatment recommended by your physician or a tobacco cessation program). If you use tobacco and want to quit, SSC offers tobacco
cessation programs that are available at no cost to you. If you complete the program you will be eligible for the $100 monthly discount.
2 If your spouse is eligible for medical coverage through another employer or plan, you will pay a $100 monthly surcharge if
you enroll them in an SSC medical plan.
12 2022 Health and Benefits Guide