
Page 218 - Feline diagnostic imaging
P. 218
13.10 Dilated Cardiomyopatcy 221
(a) (c)
(b) (d)
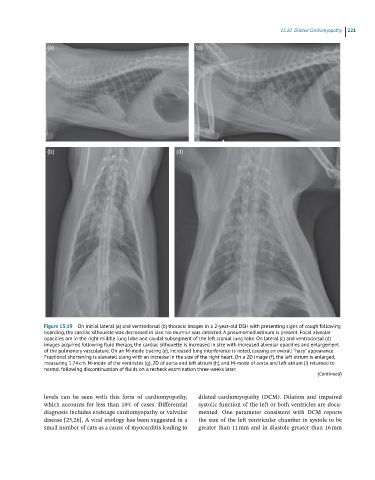
Figure 13.19 On initial lateral (a) and ventrodorsal (b) thoracic images in a 2-year-old DSH with presenting signs of cough following
boarding, the cardiac silhouette was decreased in size. No murmur was detected. A pneumomediastinum is present. Focal alveolar
opacities are in the right middle lung lobe and caudal subsegment of the left cranial lung lobe. On lateral (c) and ventrodorsal (d)
images acquired following fluid therapy, the cardiac silhouette is increased in size with increased alveolar opacities and enlargement
of the pulmonary vasculature. On an M-mode tracing (e), increased lung interference is noted, causing an overall “hazy” appearance.
Fractional shortening is elevated along with an increase in the size of the right heart. On a 2D image (f), the left atrium is enlarged,
measuring 1.74 cm. M-mode of the ventricles (g), 2D of aorta and left atrium (h), and M-mode of aorta and left atrium (i) returned to
normal following discontinuation of fluids on a recheck examination three weeks later.
(Continued)
levels can be seen with this form of cardiomyopathy, dilated cardiomyopathy (DCM). Dilation and impaired
which accounts for less than 10% of cases. Differential systolic function of the left or both ventricles are docu
diagnosis includes endstage cardiomyopathy or valvular mented. One parameter consistent with DCM reports
disease [25,26]. A viral etiology has been suggested in a the size of the left ventricular chamber in systole to be
small number of cats as a cause of myocarditis leading to greater than 11 mm and in diastole greater than 16 mm