
Page 220 - Feline diagnostic imaging
P. 220
13.12 Arrcytcmogenic igct Ventricular Cardiomyopatcy 223
(a) (b)
(c)
(d)
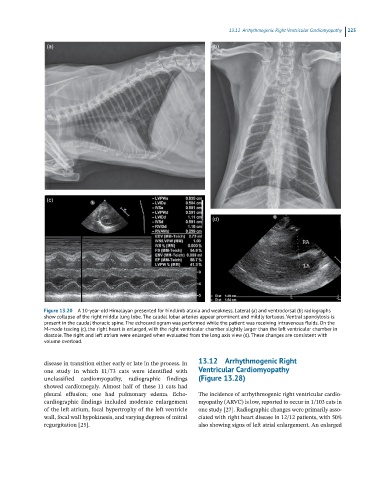
Figure 13.20 A 10-year-old Himalayan presented for hindlimb ataxia and weakness. Lateral (a) and ventrodorsal (b) radiographs
show collapse of the right middle lung lobe. The caudal lobar arteries appear prominent and mildly tortuous. Ventral spondylosis is
present in the caudal thoracic spine. The echocardiogram was performed while the patient was receiving intravenous fluids. On the
M-mode tracing (c), the right heart is enlarged, with the right ventricular chamber slightly larger than the left ventricular chamber in
diastole. The right and left atrium were enlarged when evaluated from the long axis view (d). These changes are consistent with
volume overload.
disease in transition either early or late in the process. In 13.12 Arrhythmogenic Right
one study in which 11/73 cats were identified with Ventricular Cardiomyopathy
unclassified cardiomyopathy, radiographic findings (Figure 13.28)
showed cardiomegaly. Almost half of these 11 cats had
pleural effusion; one had pulmonary edema. Echo The incidence of arrhythmogenic right ventricular cardio
cardiographic findings included moderate enlargement myopathy (ARVC) is low, reported to occur in 1/103 cats in
of the left atrium, focal hypertrophy of the left ventricle one study [27]. Radiographic changes were primarily asso
wall, focal wall hypokinesis, and varying degrees of mitral ciated with right heart disease in 12/12 patients, with 50%
regurgitation [25]. also showing signs of left atrial enlargement. An enlarged