
Page 17 - textbook5chapters
P. 17
1038 Surgical Anatomy in Pelvic Gynaecologic Oncology
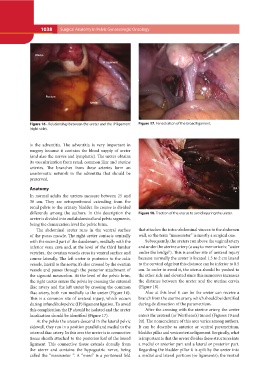
Figure 16 . Relationship between the ureter and the IP ligament Figure 17. Fenestration of the broad ligament.
(right side).
is the adventitia. The adventitia is very important in Figure 18. Traction of the uterus to avoid injuring the ureter.
surgery because it contains the blood supply of ureter
(and also the nerves and lymphatic). The ureter obtains that attaches the intra-abdominal viscera to the abdomen
its vascularization from renal, common iliac and uterine wall, so the term “mesoureter” is mostly a surgical one.
arteries. The branches from these arteries form an
anastomotic network in the adventitia that should be Subsequently, the ureters run above the vaginal artery
preserved. and under the uterine artery (a way to memorize is: “water
under the bridge”). This is another site of ureteral injury
Anatomy because normally the ureter is located 1.5 to 2 cm lateral
to the cervical edge but this distance can be inferior to 0.5
In normal adults the ureters measure between 25 and cm. In order to avoid it, the uterus should be pushed to
30 cm. They are retroperitoneal extending from the the other side and elevated since this maneuver increases
renal pelvis to the urinary bladder. Its course is divided the distance between the ureter and the uterine cervix
differently among the authors. In this description the (Figure 18).
ureter is divided into and abdominal and pelvic segments,
being the demarcation level the pelvic brim. Also at this level it can be the ureter can receive a
branch from the uterine artery, which should be identified
The abdominal ureter runs in the ventral surface during de dissection of the parametrium.
of the psoas muscle. The right ureter contacts ventrally
with the second part of the duodenum, medially with the After the crossing with the uterine artery, the ureter
inferior vena cava and, at the level of the third lumbar enters the ureteral (or Wertheim’s) tunnel (Figures 19 and
vertebra, the ovarian vessels cross its ventral surface and 20). The nomenclature of this area varies among authors.
course laterally. The left ureter is posterior to the colic It can be describe as anterior or ventral parametrium,
vessels, lateral to the aorta; it’s also crossed by the ovarian bladder pillar and vesicouterine ligament. Surgically, what
vessels and passes through the posterior attachment of is important is that the ureter divides these structures into
the sigmoid mesocolon. At the level of the pelvic brim, a medial or anterior part and a lateral or posterior part.
the right ureter enters the pelvis by crossing the external Regarding the bladder pillar it is split by the ureter into
iliac artery and the left ureter by crossing the common a medial and lateral portions (or ligaments); the ventral
iliac artery, both run medially to the ureter (Figure 16).
This is a common site of ureteral injury, which occurs
during infundibulopelvic (IP) ligament ligation. To avoid
this complication the IP should be isolated and the ureter
localization should be identified (Figure 17).
At the pelvis the ureters descend in the lateral pelvic
sidewall, they run in a position parallel and medial to the
internal iliac artery. In this area the ureter is in connective
tissue sheath attached to the posterior leaf of the broad
ligament. This connective tissue extends dorsally from
the uterer and contains the hypogastric nerve, being
called the “mesoureter “. A “meso” is a peritoneal fold