
Page 73 - Small Animal Internal Medicine, 6th Edition
P. 73
CHAPTER 2 Diagnostic Tests for the Cardiovascular System 45
VetBooks.ir
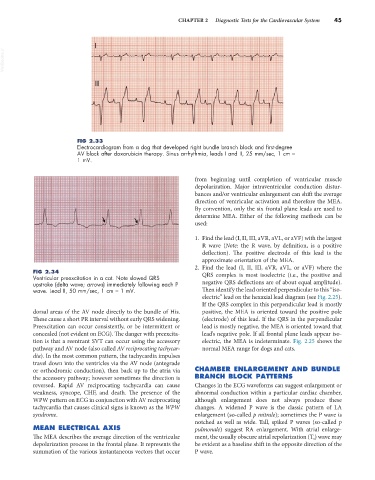
FIG 2.33
Electrocardiogram from a dog that developed right bundle branch block and first-degree
AV block after doxorubicin therapy. Sinus arrhythmia, leads I and II, 25 mm/sec, 1 cm =
1 mV.
from beginning until completion of ventricular muscle
depolarization. Major intraventricular conduction distur-
bances and/or ventricular enlargement can shift the average
direction of ventricular activation and therefore the MEA.
By convention, only the six frontal plane leads are used to
determine MEA. Either of the following methods can be
used:
1. Find the lead (I, II, III, aVR, aVL, or aVF) with the largest
R wave (Note: the R wave, by definition, is a positive
deflection). The positive electrode of this lead is the
approximate orientation of the MEA.
2. Find the lead (I, II, III, aVR, aVL, or aVF) where the
FIG 2.34 QRS complex is most isoelectric (i.e., the positive and
Ventricular preexcitation in a cat. Note slowed QRS
upstroke (delta wave; arrows) immediately following each P negative QRS deflections are of about equal amplitude).
wave. Lead II, 50 mm/sec, 1 cm = 1 mV. Then identify the lead oriented perpendicular to this “iso-
electric” lead on the hexaxial lead diagram (see Fig. 2.25).
If the QRS complex in this perpendicular lead is mostly
dorsal areas of the AV node directly to the bundle of His. positive, the MEA is oriented toward the positive pole
These cause a short PR interval without early QRS widening. (electrode) of this lead. If the QRS in the perpendicular
Preexcitation can occur consistently, or be intermittent or lead is mostly negative, the MEA is oriented toward that
concealed (not evident on ECG). The danger with preexcita- lead’s negative pole. If all frontal plane leads appear iso-
tion is that a reentrant SVT can occur using the accessory electric, the MEA is indeterminate. Fig. 2.25 shows the
pathway and AV node (also called AV reciprocating tachycar- normal MEA range for dogs and cats.
dia). In the most common pattern, the tachycardia impulses
travel down into the ventricles via the AV node (antegrade
or orthodromic conduction), then back up to the atria via CHAMBER ENLARGEMENT AND BUNDLE
the accessory pathway; however sometimes the direction is BRANCH BLOCK PATTERNS
reversed. Rapid AV reciprocating tachycardia can cause Changes in the ECG waveforms can suggest enlargement or
weakness, syncope, CHF, and death. The presence of the abnormal conduction within a particular cardiac chamber,
WPW pattern on ECG in conjunction with AV reciprocating although enlargement does not always produce these
tachycardia that causes clinical signs is known as the WPW changes. A widened P wave is the classic pattern of LA
syndrome. enlargement (so-called p mitrale); sometimes the P wave is
notched as well as wide. Tall, spiked P waves (so-called p
MEAN ELECTRICAL AXIS pulmonale) suggest RA enlargement. With atrial enlarge-
The MEA describes the average direction of the ventricular ment, the usually obscure atrial repolarization (T a ) wave may
depolarization process in the frontal plane. It represents the be evident as a baseline shift in the opposite direction of the
summation of the various instantaneous vectors that occur P wave.