
Page 584 - Feline diagnostic imaging
P. 584
598 32 Overview of the Musculoskeletal System
Figure 32.27 Lateral (a) and craniocaudal (b) views of the
humerus. Ballistic injury to the distal diaphysis of the humerus
causing multiple fractures is noted. Because this is a ballistic
injury, the fracture is considered open despite the absence of
obvious gas opacities in the soft tissues.
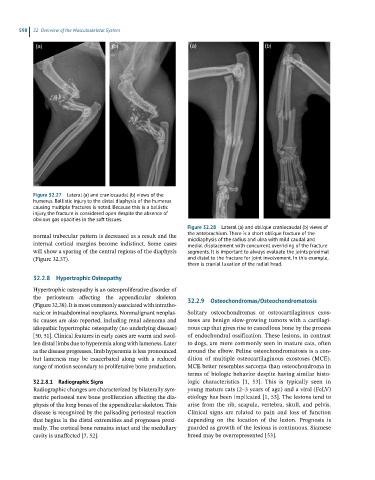
Figure 32.28 Lateral (a) and oblique craniocaudal (b) views of
normal trabecular pattern is decreased as a result and the the antebrachium. There is a short oblique fracture of the
middiaphysis of the radius and ulna with mild caudal and
internal cortical margins become indistinct. Some cases medial displacement with concurrent overriding of the fracture
will show a sparing of the central regions of the diaphysis segments. It is important to always evaluate the joints proximal
(Figure 32.37). and distal to the fracture for joint involvement. In this example,
there is cranial luxation of the radial head.
32.2.8 Hypertrophic Osteopathy
Hypertrophic osteopathy is an osteoproliferative disorder of
the periosteum affecting the appendicular skeleton 32.2.9 Osteochondromas/Osteochondromatosis
(Figure 32.38). It is most commonly associated with intratho-
racic or intraabdominal neoplasms. Nonmalignant neoplas- Solitary osteochondromas or osteocartilaginous exos-
tic causes are also reported, including renal adenoma and toses are benign slow-growing tumors with a cartilagi-
idiopathic hypertrophic osteopathy (no underlying disease) nous cap that gives rise to cancellous bone by the process
[50, 51]. Clinical features in early cases are warm and swol- of endochondral ossification. These lesions, in contrast
len distal limbs due to hyperemia along with lameness. Later to dogs, are more commonly seen in mature cats, often
as the disease progresses, limb hyperemia is less pronounced around the elbow. Feline osteochondromatosis is a con-
but lameness may be exacerbated along with a reduced dition of multiple osteocartilaginous exostoses (MCE).
range of motion secondary to proliferative bone production. MCE better resembles sarcoma than osteochondroma in
terms of biologic behavior despite having similar histo-
32.2.8.1 Radiographic Signs logic characteristics [1, 53]. This is typically seen in
Radiographic changes are characterized by bilaterally sym- young mature cats (2–3 years of age) and a viral (FeLV)
metric periosteal new bone proliferation affecting the dia- etiology has been implicated [1, 53]. The lesions tend to
physis of the long bones of the appendicular skeleton. This arise from the rib, scapula, vertebra, skull, and pelvis.
disease is recognized by the palisading periosteal reaction Clinical signs are related to pain and loss of function
that begins in the distal extremities and progresses proxi- depending on the location of the lesion. Prognosis is
mally. The cortical bone remains intact and the medullary guarded as growth of the lesions is continuous. Siamese
cavity is unaffected [7, 52]. breed may be overrepresented [53].