
Page 514 - Adams and Stashak's Lameness in Horses, 7th Edition
P. 514
480 Chapter 4
VetBooks.ir
A B B
Figure 4.48. Dorsopalmar (A) and lateral radiographs (B) of the feet in two adult horses with severe lameness due to infection of the distal
phalanx. Osteolysis of the solar surface (A; arrow) and extensor process (B; arrow) of the distal phalanx is evident consistent with infection.
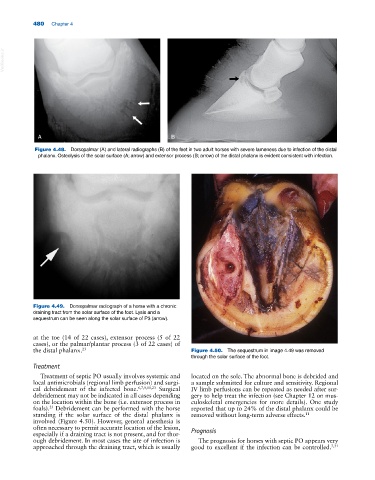
Figure 4.49. Dorsopalmar radiograph of a horse with a chronic
draining tract from the solar surface of the foot. Lysis and a
sequestrum can be seen along the solar surface of P3 (arrow).
at the toe (14 of 22 cases), extensor process (5 of 22
cases), or the palmar/plantar process (3 of 22 cases) of
the distal phalanx. 23 Figure 4.50. The sequestrum in image 4.49 was removed
through the solar surface of the foot.
Treatment
Treatment of septic PO usually involves systemic and located on the sole. The abnormal bone is debrided and
local antimicrobials (regional limb perfusion) and surgi- a sample submitted for culture and sensitivity. Regional
cal debridement of the infected bone. 6,7,9,11,23 Surgical IV limb perfusions can be repeated as needed after sur-
debridement may not be indicated in all cases depending gery to help treat the infection (see Chapter 12 on mus-
on the location within the bone (i.e. extensor process in culoskeletal emergencies for more details). One study
foals). Debridement can be performed with the horse reported that up to 24% of the distal phalanx could be
23
standing if the solar surface of the distal phalanx is removed without long‐term adverse effects. 11
involved (Figure 4.50). However, general anesthesia is
often necessary to permit accurate location of the lesion,
especially if a draining tract is not present, and for thor- Prognosis
ough debridement. In most cases the site of infection is The prognosis for horses with septic PO appears very
approached through the draining tract, which is usually good to excellent if the infection can be controlled. 7,31