
Page 294 - Essential Haematology
P. 294
280 / Chapter 21 Multiple myeloma and related disorders
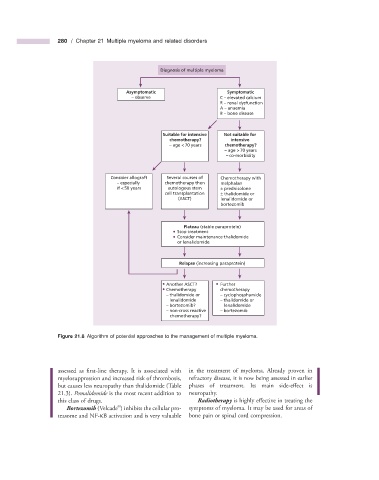
Diagnosis of multiple myeloma
Asymptomatic Symptomatic
– observe C – elevated calcium
R – renal dysfunction
A – anaemia
B – bone disease
Suitable for intensive Not suitable for
chemotherapy? intensive
– age < 70 years chemotherapy?
– age > 70 years
– co-morbidity
Consider allograft Several courses of Chemotherapy with
– especially chemotherapy then melphalan
if < 50 years autologous stem ± prednisolone
cell transplantation ± thalidomide or
(ASCT) lenalidomide or
bortezomib
Plateau (stable paraprotein)
Stop treatment
Consider maintenance thalidomide
or lenalidomide
Relapse (increasing paraprotein)
Another ASCT? Further
Chemotherapy chemotherapy
– thalidomide or – cyclophosphamide
lenalidomide – thalidomide or
– bortezomib? lenalidomide
– non-cross reactive – bortezomib
chemotherapy?
Figure 21.8 Algorithm of potential approaches to the management of multiple myeloma.
assessed as first - line therapy. It is associated with in the treatment of myeloma. Already proven in
myelosuppression and increased risk of thrombosis, refractory disease, it is now being assessed in earlier
but causes less neuropathy than thalidomide (Table phases of treatment. Its main side - eff ect is
21.3 ). Pomalidomide is the most recent addition to neuropathy.
this class of drugs. Radiotherapy is highly effective in treating the
®
Bortezomib (Velcade ) inhibits the cellular pro- symptoms of myeloma. It may be used for areas of
teasome and NF - κ B activation and is very valuable bone pain or spinal cord compression.