
Page 53 - Essential Haematology
P. 53
Chapter 3 Hypochromic anaemias / 39
Fe 3+ Fe 2+ Haem
DMT-1
Ferrireductase
Haem
oxygenase
Ferritin
Mitochondrion
Ferroportin
Hepcidin Ferrioxidase
Fe 3+
Transferrin
Portal
plasma
2 +
3 +
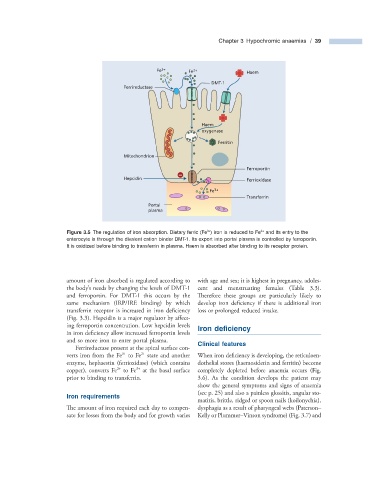
Figure 3.5 The regulation of iron absorption. Dietary ferric (Fe ) iron is reduced to Fe and its entry to the
enterocyte is through the divalent cation binder DMT - 1. Its export into portal plasma is controlled by ferroportin.
It is oxidized before binding to transferrin in plasma. Haem is absorbed after binding to its receptor protein.
amount of iron absorbed is regulated according to with age and sex; it is highest in pregnancy, adoles-
the body s needs by changing the levels of DMT - 1 cent and menstruating females (Table 3.3 ).
’
and ferroportin. For DMT - 1 this occurs by the Th erefore these groups are particularly likely to
same mechanism (IRP/IRE binding) by which develop iron deficiency if there is additional iron
transferrin receptor is increased in iron defi ciency loss or prolonged reduced intake.
(Fig. 3.3 ). Hepcidin is a major regulator by aff ect-
ing ferroportin concentration. Low hepcidin levels Iron d efi ciency
in iron deficiency allow increased ferroportin levels
and so more iron to enter portal plasma. Clinical f eatures
Ferrireductase present at the apical surface con-
3 +
2 +
verts iron from the Fe to Fe state and another When iron defi ciency is developing, the reticuloen-
enzyme, hephaestin (ferrioxidase) (which contains dothelial stores (haemosiderin and ferritin) become
3 +
2 +
copper), converts Fe to Fe at the basal surface completely depleted before anaemia occurs (Fig.
prior to binding to transferrin. 3.6 ). As the condition develops the patient may
show the general symptoms and signs of anaemia
(see p. 25 ) and also a painless glossitis, angular sto-
Iron r equirements
matitis, brittle, ridged or spoon nails (koilonychia),
The amount of iron required each day to compen- dysphagia as a result of pharyngeal webs (Paterson –
sate for losses from the body and for growth varies Kelly or Plummer – Vinson syndrome) (Fig. 3.7 ) and